
I have recently discussed in detail the rapidly increasing costs of American healthcare.
I have suggested ways in which the costs of our public healthcare programs, Medicare and Medicaid, can be controlled.
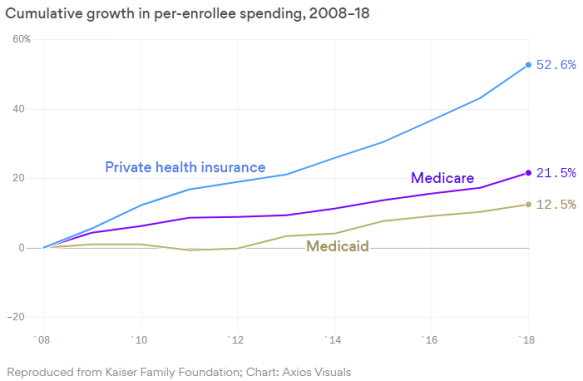
But the cost of private healthcare is increasing even faster than for the public programs. For example, the cost of Medicare has increased by 21.5% in the last ten years, the cost of Medicaid has increased by 12.5% while the cost of private insurance has increased by 52.6%.
The International Federation of Health Plans (iFHP) has clearly described the high costs of American healthcare compared to other countries. For example:
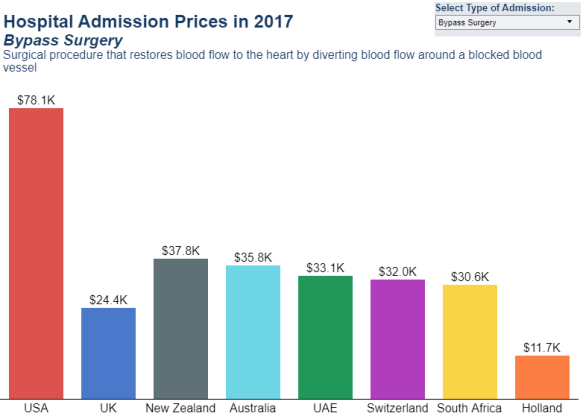
- Bypass surgery was less than half the price for the U.S. in all the other countries included in the study (see below).

- The average cost of bypass surgery in the U.S. is $78,000 while the second highest cost (New Zealand) is $37,800 (see below).
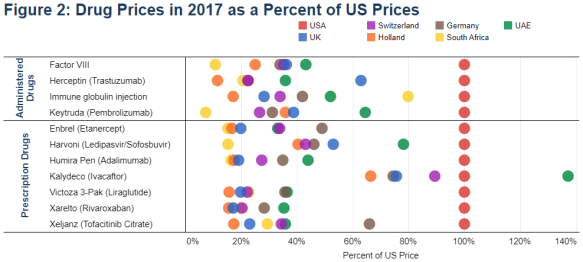
- Drug prices for most countries were less than half the U.S. price for almost all of the administered and prescription drugs included in the study (see below).
How are these exorbitant prices for private American healthcare being paid? It turns out that individual company employees are paying gradually increasing out-of-pocket costs (premiums and deductibles). But primarily it is employers who are paying the major share of the increased costs. Of course, this means that base employee salaries and wages are substantially less as a result (see below).
Conclusion. The cost of American healthcare is much too high for both individuals and the government. The rapidly increasing federal government costs are the primary cause of our rapidly increasing annual deficits and therefore to our out-of-control national debt. Private healthcare cost increases are largely paid for by employers which means less pay for employees.
So far only Medicare and Medicaid have been able to exert any meaningful cost control and this has been done with strict price controls. It is unlikely that private companies will be able to develop the clout to limit their healthcare costs in any significant way. This means that overall strict price controls for all of U.S. healthcare are almost inevitable.

The wide divergence of health spending by payer reveals a dramatic worsening after the introduction of ACA 2010 (Obamacare in 2013-14). Since the private payer contracts between the providers of complex healthcare and the private payers of this healthcare are “trade secrets,” the divergence merely represents a form of Parkinson’s Law. It is most widely recognized as “work expands to use the resources available.” I also believe that the law of unintended results applies. The fragile funding of medical education is poorly recognized, especially recognizable by the very high debt-load of most under-graduate and post-graduate medical students. Is it possible that this debt-load skews the general character of medical school applicants? Maybe…maybe not.
I should also observe that the political capital associated with price controls may adversely affect more pressing reform needs of our nation’s healthcare. Basically, the long-standing lack of adequate funding for Primary Healthcare by Medicare and Medicaid put my practice out of business in 2016. You really can’t offer adequate medical Triage for Primary Healthcare without employing a small staff of BSN level nurses to answer the office phone for accessibility. Good nurses should be considered as the baseline strategy to improve health spending by enhanced Primary Healthcare. Remember the core professional identity of a good nurse is defined by the ability to help each patient improve their HEALTH through a high-quality caring relationship.
The high cost of medical school and how to pay for it is a problem but it should be solved separately rather than bogging down the effort to get overall healthcare costs under control.
I understand the value of using BSN level nurses to offer adequate medical triage for primary healthcare. But this should be considered as a cost saving measure by achieving better health outcomes.
Columbus (NE) Community Hospital (https://www.columbushosp.org/) has apparently figured out how to succeed financially with Medicare and Medicaid level reimbursements.
The financial stability of a hospital’s capitalization takes hard work and leadership. However, it doesn’t necessarily translate to over-all health spending. The Medicare folks have defined referral regions from which many persons receive complex healthcare at a large regional metropolitan area’s medical center. For Northeast and Central Nebraska north of the Platte River, the most common medical center for Medicare Complex Healthcare is the University of Nebraska Medical Center. Southeast and Central Nebraska south of the Platte River is connected to Lincoln or the Creighton University Hospital (currently at CHI Bergan). Given health spending for Nebraska in 2017 at just over $10,000 per resident person AND assuming that $3,000 is excess, Nebraska has excess health spending at $6 billion. Assuming that 50% of the excess is paid by the Federal Government, the other $3 billion is paid by resident persons, employers, and local/state taxes. Just think what could happen to employment training, infra-structure maintenance, and early childhood education with $1 billion (the other $2 Billion allocated to reduced taxes).
No doubt, CEO Michael Hansen at Columbus Community Hospital is providing excellent leadership in holding down medical costs at his hospital. But if he can do it, other hospitals and medical providers should also be able to do this.
Just because $3000 is wasted out of the total cost of $10,000 per person in healthcare spending for Nebraskans, I suspect that it would be exceeding difficult (essentially impossible) even to identify let alone eliminate this enormous amount of waste in the system.
To me it makes more sense for third party payers to reduce their payments by 30% or so (the amount of theoretical waste you estimate) and then expect the providers to make this up by ferreting out the waste themselves.
The economist Ewe Rinehardt staked his career upon the same proposition. I would add that health spending represents a paradox in that its solution will likely involve difficult and variously unacceptable economic changes in national priorities. Such is the character of our times.
I have absolutely no doubt that what we are agreeing on here will be very difficult for he healthcare industry to implement. But first we (you and I and many others) have to figure out and agree on what needs to be done and then push for its implementation.
In other words, we want to make sure that, regardless of the difficulty of success. we are at least moving in the right direction.