
One of the major topics I discuss on this blog is:
- Economic growth, in particular the fact that the U.S. economy has grown at the relatively slow rate of 2.1% per year since the end of the Great Recession in June 2009. It appears, however, that the economy may now be starting to pick up speed.
There are plenty of “experts” who say that it is unrealistic to expect economic growth to continue indefinitely at the same level (3% on average) which has prevailed since the end of WWII because:
- Resources are limited. The earth is finite but it is also vast. It is unlikely that any mineral or even energy source such as fossil fuels will be depleted for hundreds, if not thousands, of years. If and when any particular resource becomes scarce, human ingenuity will be able to find a replacement.
- Population growth is slowing down. It is likely that human population worldwide will level off this century somewhere between 9 and 10 billion. This is highly desirable but is unlikely to slow down economic growth. As income and education levels rise, productivity and GDP per person will also increase.
- Growth tends to be debt financed which is unsustainable. I agree with this reservation. This is the one problem, if not solved, which has the potential to derail continued steady progress.

The remarkable human progress of the last 200 years is likely to continue indefinitely. In particular:
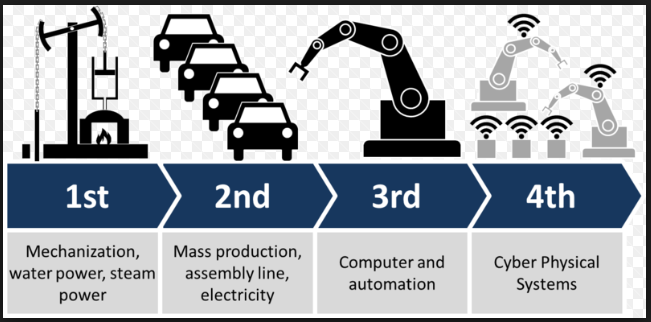
- The Fourth Industrial Revolution (succeeding the steam, electrical and digital revolutions) is now upon us. It consists of robotics, artificial intelligence, the internet of things, 3D printing, autonomous vehicles, etc. It will lead to huge increases in efficiency and productivity without making human work obsolete.
Conclusion. The world has enjoyed remarkable human progress in the last two hundred years, in the form of steady economic growth, and this progress is likely to continue indefinitely into the future.

One view of progress among the nation’s of the world would observe that our current scientific progress has not been matched by our humanitarian progress. I cite the continued occurrence of genocide, global slavery (estimated at 300 million by a September 2017 LA Times report), continued threat of nuclear war, the world-wide black market for narcotics, 86% of the world’s population lives in a Nation without our First Amendment Rights, and the effect of our burgeoning loss of internet safety on our own First Amendment Rights. Finally, we lack a well accepted strategy to sustain a community by community commitment to maintain the COMMON GOOD for the citizens of each community. As the most advanced Nation of the world, we are the only developed nation with a worsening level of maternal mortality, for 25 years in a row.
But isn’t it to be expected that humanitarian progress will lag economic progress? Humanity is better off today than it was 100 years ago and was better off in 1917 (except for WWI!) than it was in 1817.
Overall, it seems to me, there is a steady march of progress.
So, a Machiavellian strategy continues, since 1579, to dominate our world’s international relationships using mass extinction as the ultimate threat. The United Nations really only functions as an “at-a-boy” forum for these issues. The ongoing cognitive dissonance between the humanitarian and scientific realms of knowledge continues unabated, in some ways worsening since the origins of the Christian Reformation 500 years ago, as of today. Let’s be clear that a person’s family, neighborhood and their community are the origins of our HEALTH and well-being. To the extent that our nation supports the equitable, ecologic, just and reliable attributes of the COMMON GOOD for each citizen’s community, we will have achieved equipoise between our realms of scientific and humanitarian KNOWLEDGE. I would judge that its a millennium beyond the horizon, depending on the resolution of global warming or an asteroid collision.
.
On a more positive note, the Design Principles for managing a common-pool resource (as in, our National economy) have already been defined and largely validated. Nobel Prize winner Elinor Ostrom, 2009, is their original author.
Where I think we differ is on how we get from here (where we are today) to there (the Common Good). I believe that we are already getting, and will continue to get, closer to the Common Good by a natural process of social evolution, even though progress certainly does not proceed in a straight line. (Trump is a setback, for example).
I think you are somewhat impatient and would like to speed up the process somehow. As long as we are moving in the right direction overall (as I think we are), this is probably the best we can do.
By the way, according to Elinor Ostom’s design principles, what is the very next step or two that we should be trying o take right now?
The first step would require Congress to Charter a new, semi-autonomous institution, similar to the Federal Reserve (chartered in 1913) with a mandate to lower health spending to 13% of the GDP and lower the maternal mortality ratio from 23.8 in 2014 to 10.0 or less within 10 years. The new institution would be governed by a Board of Trustees of 9 members, each from a regional portion of the United States comprised of @ 36 million citizens. The Members would each serve 9 years on an annual rotating basis, with the Board of Trustees as a group, having certain expertise: Primary Physicians – 3, Sub-Specialist Physician – 1; Academic Physician with curriculum expertise – 1; Public Health non-Physician – 1; Mental Health Non-Physician – 1; Consulting Medical Ethicist – 1; “Professional” Community volunteer – 1. This institution would be funded by $1.00 per citizen per year, face a 10 years scenario to attain its mandate, and managed by a 4 levels of increasing decentralization ending with @ 800 Health Forums each responsible for, on average, 400,000 citizens each. The local groups would be self funded with technical support by the Chartered institution. The local groups would governed by a small group of key local Stakeholders with a responsibility to assure that 1) their citizens have equitably available, ecologically accessible, justly efficient and reliably effective Primary Healthcare, the community is actively mobilizing its Social Capital to ameliorate the social adversities encumbering the HEALTH of its citizens, and 3) annually review the community’s Master Disaster Mitigation Strategy for the disasters likely to occur within next 30-60 years.
.
The Board of Trustees would directly implement its decentralized governance as supported by three national projects: 1) a set of CPT billing codes for use by ALL Payers for the reimbursement of Primary Healthcare including their definitions; 2) a regionalized, National Plan for the career-long, graduate and post-graduate education of Primary Physicians; and 3) a Primary Healthcare certification process as a means to qualify for augmented reimbursement of its services.
.
The Design Principles mainly apply to a balance between the local leadership to promote high quality Primary Healthcare clinics that are individually willing to assume responsibility for managing a meaningful but sensible-portion of the financial risk involving the cost of their citizens healthcare. Obviously, this would represent a major shift in the responsibility within our nation’s healthcare industry. Ultimately, one scenario is as follows: primary physician group assumes full risk for each patient up to $70,000 billable charges for any citizen during a calendar year; the payer from $70,001 – $150,000; the citizen’s state risk-fund for $150,001 through $3 Million; and the Federal government for >$3,000.000. Basically, the specialist physicians would be paid fee for service (including a with-hold) or pre-paid. Primary Physicians would be paid fee for service until Certified, then paid fee-for-service with a negotiated monthly capitation to slowly develop confidence in the stability of their risk-sharing arrangement. The confidence of both the physicians and their community’s citizens to develop relationships based on COOPERATION, RECIPROCITY and TRUST will determine the pace of conversion to risk-sharing reimbursement for healthcare. For Primary Healthcare, increased funding will be required to meaningfully manage the day to day medical triage of their citizen-patients. This level of services will require fully trained registered nurses with applicable experience.
.
The eventual leadership governance would require the Board of Trustees, 9 Regional Councils in an advice and consent relationship with the Board of Trustees (each associated with @35 Million citizens) as well as appointing one member on the Board of Trustees, 81 District Coalitions (9 for each Regional Council) representing @ 4 Million citizens each to provide technical assistance to 9-10 Health Forums and appoint one member for their Regional Council; and 9-10 Health FORUMS for each District Coalition with responsibilities noted above and nominate 2-3 persons for consideration as 1 member of their District Coalition. Along with administrative staff, nearly 1,000 persons would be involved, 80% locally supported.
.
The Design Principles eventually shade how well the Institution is able to regionally capitalize its direct healthcare services through its association with defining the reimbursable units, the regionalized career-long training process including its association with clinic certification for Primary Healthcare, and the promotion of the COMMON GOOD within each community that is locally driven. With the ten year “drop-dead” envelope, the obligation of the initial Board of Trustees to build trusting relationships with each State will be imperative for achieving the 10 year goal. It would be slow for the first 5 years, then gain momentum based ultimately on the level of Social Capital that occurs within each community. As a basically disruptive process within our nation, the Board of Trustees will require a very high level of sensitivity to avoid conflict of interests and to communicate, communicate and communicate. In short, a carefully defined risk management plan will be required, trained and tested.
see https://nationalhealthusa.net/summary/
Thanks for the outline which I understand in a general sense except for the payment scheme. I assume our current funding scheme (employer provided insurance, Medicare, Medicaid, etc) is somehow modified but what form will it take?