
One of the very most serious problems facing our nation is our massive federal debt, now over $13 trillion (the public debt on which we pay interest), or 75% of GDP, the highest since right after WWII, and predicted by the CBO to keep getting worse unless major policy changes are made.
The main contributors to this rising debt are the big three entitlement programs of Social Security, Medicare and Medicaid. All three need substantial reforms in order to rein in spending.
Today I will discuss Medicaid, based on an excellent analysis performed by the Manhattan Institute’s Oren Cass, “Over-Medicaid-Ed: how Medicaid distorts and dilutes America’s Safety net.”
 Consider these pertinent points:
Consider these pertinent points:
- Badly designed incentives for Medicaid expansion. Each state sets the size of its Medicaid program and receives matching federal dollars, from $1 to $4, for every dollar spent. States thus have a strong incentive to overinvest in Medicaid, expanding their programs far beyond the point where a marginal dollar of their own spending produces a dollar of value.
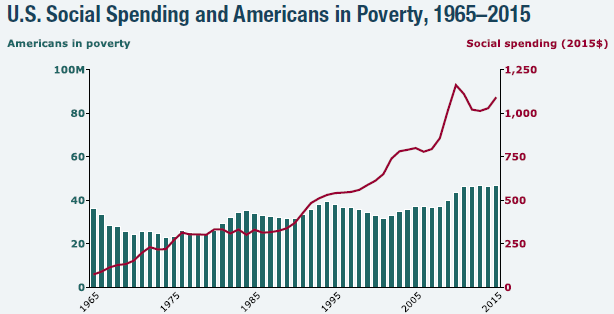
- Health care dominates safety-net spending. During 1975 – 2015, government social spending per person in poverty more than doubled (in constant 2015 dollars) from $11,600 to $23,400. Rising health care expenditures accounted for more than 90% of that increase.
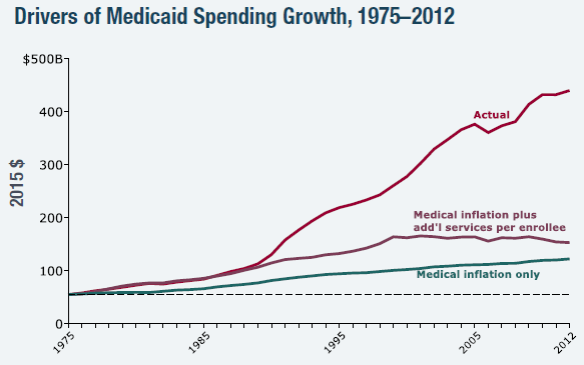
- Medicaid spending in 2012 was 39% higher than if it had remained a constant share of state budgets since 2000. State spending on education and welfare was 9% and 54% lower, respectively.
- This allocation is an ineffective poverty-fighting strategy. While the majority of government social spending goes to health care, low-income households not enrolled in Medicaid allocate less than 10% of their spending to health care. Studies consistently show little or no positive impact on health outcomes from Medicaid enrollment.
- How to strengthen America’s safety net. The federal government should consolidate all antipoverty funding streams, including Medicaid, and allow states to design programs and allocate funding to such programs as states see fit.

Conclusion. The above program outlines a way to both improve the effectiveness of social welfare spending and curtail its costs to both states and the federal government. Let’s do it!
Follow me on Twitter
Follow me on Facebook

Jack,
There just doesn’t seem to be much concern about the high cost of our nation’s healthcare. Its almost 10:30 pm CDST and no comments until now. In the three other health reform Blogs that I follow, the same occurs. I leave a comment about it and no response. In fact, my comments were locked out by one of these Blogs, a badge of honor for me. So, let me project that in two years, the next recession will begin to evolve. On average, our recessions occur every ten years. We are now 8 years since the last one. What if three large healthcare systems suddenly became insolvent and closed? Then what? Well, of course, Federal loan guarantees. I’d be interested in your readers best guess about what would happen next after the loan guarantees.
The point of this WHAT IF really reflects the lack of any current discussion about the possible strategies that might realistically resolve the fundamental paradigm paralysis of our nation’s healthcare industry. I will check back tomorrow to see if anyone else is really concerned about it.
Paul
I agree with you that the next recession, which could well come in just a few years, will cause a lot of financial pain.
This is why we should reform health care now instead of waiting until a crisis occurs. I think there is a good way to proceed, as I described in a previous post: https://itdoesnotaddup.com/2016/08/23/how-to-improve-obamacare-and-lower-its-costs/.
A simplified version of this plan is to just modify the ACA by eliminating the mandates and keeping the exchanges.
I guess that I’m more optimistic than you are about fixing American health care. I think it can be done and I suspect it will be done one way or another.
Jack,
I see that no one else has risen to the occasion. I continue to believe that Parkinson’s Law has led to a paradigm paralysis of our nation’s healthcare industry. Maybe the next recession will bring about a renewed energy for meaningful change…or maybe not, too!
Paul
You may be right, of course. It is very difficult to make big changes without a crisis at hand. But I continue to advocate and hope for meaningful change before we have a crisis.