
It is now generally accepted that Donald Trump was elected President because of his strong support amongst white blue-collar workers, especially in the battle ground states of Wisconsin, Michigan and Pennsylvania. Mr. Trump was able to persuade these voters that he would be able to raise their stagnant incomes and even bring back the millions of manufacturing jobs which have been lost to automation and globalization.

Now the two economists, Anne Case and Angus Deaton, have shown that mortality rates for white, U.S. non-Hispanics, aged 45 – 54, with a high school degree or less, have doubled since 1990.
Here is the general situation:
- Overall, U.S. life expectancy at birth has increased from 63 years in 1940 to 79 years in 2010.
- Life expectancy is still increasing for the college educated as well for U.S. Blacks and U.S. Hispanics. It is also still rising in many other developed countries.
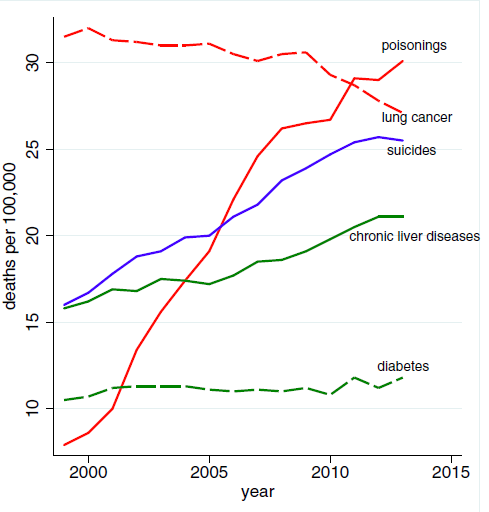
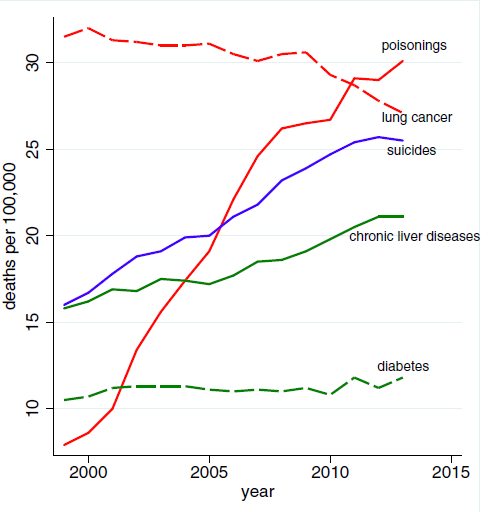
- The main cause for the rising death rates of the vulnerable group is “deaths of despair” – suicides, drug overdoses and the consequences of heavy drinking.
The authors point out that:
- It is precisely working class whites whose economic prospects have deteriorated the most in recent years, especially since the financial crisis.
- The U.S. has moved largely to defined-contribution pension plans with stock market risk in recent years whereas in Europe defined-benefit pensions are still the norm.
- The current mortality crisis bears a resemblance to the AIDS epidemic which took the lives of 650,000 Americans from 1981 – 2015. However, public awareness of the AIDS crisis was far greater than for the current mortality epidemic.
Conclusion. The basic American dream of home ownership, modest financial and job security and a bright outlook for one’s children has faded for a large class of middle-aged workers. The crisis is manifested in an increase in mortality rates for this vulnerable class. Donald Trump’s election mandate is to fix this problem but it is a tall order indeed.

Coincidentally, suicide and homicide together is now the second most common cause of death for citizens between the 1 and 25 years of age: 25% of all deaths within this age group. All of these determinants of health are community driven. Its unlikely that the cost of healthcare can be controlled without a locally sponsored commitment to improve its Common Good, community by community nation-wide. A community’s ‘social capital’ asset that is required for this takes time to mobilize. Getting started will require a “shoot the moon” strategy with a similarly national level of mobilization. Forgive my heroics, but its true.
How about addressing these community driven problems as part of the Community Health Center Program component of the ACA? There seems to be substantial funding for this program. A Community Health Center would be a natural setting for such community wide healthcare planning.
I may be confused by the terminology, but there are already two Community Health Centers in Omaha: ‘One World’ in South Omaha and ‘Charles Drew’ in North Omaha. These centers exist throughout Nebraska and the nation. The ACA substantially increased the financial support for these centers which are primarily focused on poorly served areas. Local healthcare reform should collaborate with the local institutions to improve the operating characteristics of Primary Healthcare throughout a community, no matter who originates these services: private practice, medical school, VA system, or large health enterprises.
Is there an overall institutional structure and national office for Community Health Centers? If so, wouldn’t this be the place to conduct research on national health needs? An office which spends several billion dollars a year has to have some sort of coherent organizational structure.