
On January 24 I announced my candidacy in the Republican Primary for U.S. Senate against the incumbent Deb Fischer who is doing nothing to reduce our badly out-of-control national debt and, in fact, just voted to increase it by $1 trillion over the next decade.
It is the high cost of government healthcare spending for Medicare, Medicaid and the tax exemption for employer-provided care which is the main driver of federal debt.
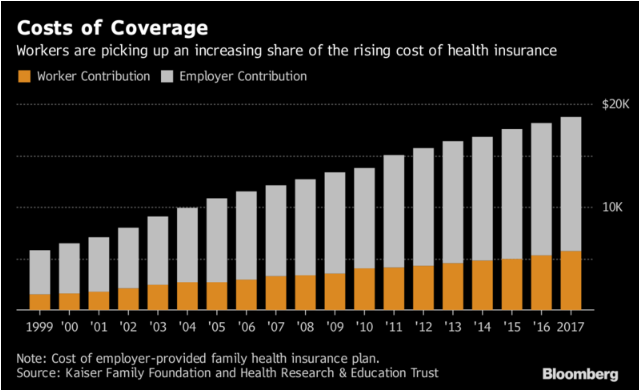
But now look at a recent report from Bloomberg Markets on the outrageously high cost of employer-provided health insurance for American workers:
- The average worker paid $5,714 in 2017 out of a total cost of $18,764 for a family plan. Deductibles last year averaged $5,950 per individual and double that per family.
- In the past five years insurance premiums increased by 19% while worker pay increased by 12% and inflation increased by just 6%.
- A family of four paid $26,944 for healthcare expenses (including out-of-pocket) last year which was 44% of median household income of $59,039.
- Health insurance premiums are up 11% in 2018.
Conclusion. I have been predicting a fiscal crisis in the relatively near future over federal debt. But we actually have an immediate crisis on our hands over the horrendous cost of employer-provided healthcare.

OK, one more time. We will need three strategies: 1) Our nation will require a nationally sanctioned strategy to establish a locally driven process to assure that equitable available, enhanced Primary Healthcare is offered to each of its citizens through a collective thrust process involving each community’s local stakeholders, 2) Our nation will require a concurrent strategy that uses the collective thrust process established for Primary Healthcare to mobilize locally defined projects to improve the local deficits in Social Capital and Social Mobility, and 3) a counter-balance to the long enduring adverse effects of Parkinson’s Law will require a renewal of financial risk-sharing distribution between the Federal government, State government, Health Insurance Institutions, Hospitals, Complex Healthcare Providers, Basic Healthcare Providers, and each citizen based on their individual level of disposable annual income. It should be implemented during 2018.
See http://www.nationalhealthusa.net/home/rationale/
for a model to implement this strategy for a Federal expense of $1.00 per citizen per year beginning within 6 months of Congressional authorization. Remember, the ‘health spending’ EXCESS expense to the Federal government in 2016 was $400 Billion, representing 80% of the Federal Deficit that year. This will require the focus of another “Shoot the moon” commitment.
Thanks Jack for your level of personal commitment to reducing our nation’s spending habits.
Does the Affordable Care Act have a mechanism to implement the changes you are talking about? If so, that would be a convenient way to move ahead on this.
No, especially for any process to follow decentralized governance.