
In my last post, “Annual Deficits are Starting to go Back Up,” I refer to a new report from the Congressional Budget Office to show that it is the large annual increases in federal healthcare spending (Medicare, Medicaid, CHIP and Obamacare) which is the main driver of our annual deficit spending which is going to start increasing again unless we do something serious about it.
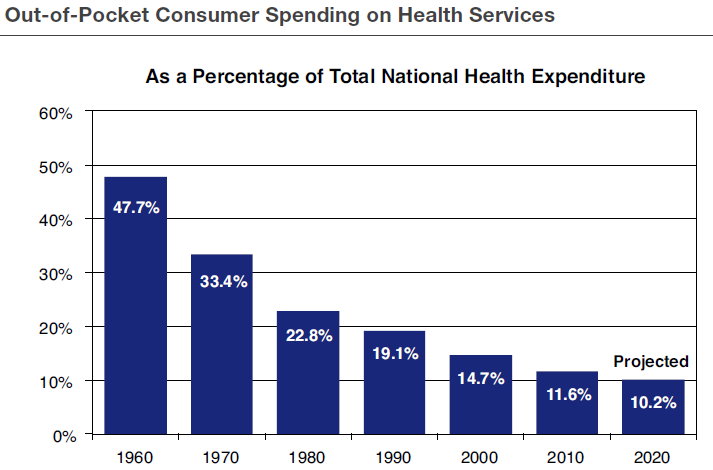 The basic problem is, as shown by the above chart, that Americans, in general, don’t have enough skin in the healthcare game, i.e. we don’t pay enough of our health care expenses out of our own pockets, and therefore we don’t directly feel the pain of high and rapidly increasing health care costs.
The basic problem is, as shown by the above chart, that Americans, in general, don’t have enough skin in the healthcare game, i.e. we don’t pay enough of our health care expenses out of our own pockets, and therefore we don’t directly feel the pain of high and rapidly increasing health care costs.
A group of policy experts from the American Enterprise Institute have come up with a practical plan to address this problem. Its elements are:
- Retain employer provided coverage. This is how half of Americans get health insurance. The only change would be an upper limit on the tax preference for employer-paid premiums so that only the most expensive plans would exceed it.
- Tax Credits. Individuals without employer coverage would get a tax credit with no strings attached to pick any state-approved plan that meets their needs.
- Continuous coverage protection. As long as people stay insured, they cannot be denied enrollment based on health status.
- Medicaid reform. The federal government would give states fixed, per-person payments based on historical spending patterns. Able bodied adult and their children could combine Medicaid and the (refundable) federal tax credit to enroll in a private insurance option.
- Medicare reform. Medicare would provide a fixed level of assistance which seniors would use to purchase a health plan of their own choosing.
- Expanded Health Savings Accounts. These are intended to be used with catastrophic insurance with a high deductible. HSAs could be established with a one-time $1000 tax credit and unused funds rolled over from one year to the next.
Such a system does not repeal, but rather improves the Affordable Care Act. It keeps the ACA exchanges and introduces cost controls in a flexible manner, i.e. without mandates. It is the type of system the U.S. needs to get health care costs, and therefore overall deficit spending, under control.
Follow me on Twitter: https://twitter.com/jack_heidel
Follow me on Facebook: https://www.facebook.com/jack.heidel.3

Jack,
This plan seems to have some merit, for it addresses all level of society as well as the individual state responsibilities. However, for such conservative states a NE and MS, I am skeptical.
Doug
This only role for the states in this AEI plan is to administer the Medicaid program with a fixed subsidy from the federal government. There’s no reason to think that the states would mess this up.
Hopefully, the state politicians will not. But as with the Affordable Care Act, services have not been reached by all citizens of the US.
Someday, you and I need to wrestle, intellectually that is, about the basic nature of being human. Also, I really would like to hear your thoughts on the essay entitled “The Case For Reparations,” by Ta-Nehisi Coates. It was in the Atlantic Monthly in 2014. David Brooks recommended it as one of the best essays of that year. I am encouraging Frank to announce it on Saturday to the two churches. I sense some reluctance on his part. But I may be wrong.
Doug
I’ve just tracked down and downloaded the Coates article and will read it promptly.
As far as the basic nature of being human, I have very much a scientific view about humanity as a product of evolution in the animal kingdom. I am also an optimist. I see humanity as progressing to higher and higher levels of well being. We’ve come long way so far and we’ll continue to improve over time assuming, of course, that the earth avoids catastrophe in the form of being hit by a giant meteor or some other event of similar scope.
See you Saturday!
Jack,
Yes, I strongly agree on the matter of evolutionary theory but see a great distinction between biological evolution and cultural evolution. In reference to history, I see more cycles than I do any clear line of moral development. So, I certainly do not have your faith in science, thus the need for philosophy and religion. Science has no morality. Its function, I understand, is to clarify what ‘is’ not what ‘ought’ to be. Nuclear energy can be used constructively or destructively. I think humans have equal access to either path. Earlier you had mentioned our progress as a people in having running water in our homes. I am not so sure that our running water in our homes has made us better people. The Romans also had that capability. Besides I never grew up having it. And, I consider my moral basis to be no better or hopefully worse than most. In one sense in matters of practicality, I knew one’s waste material had a use, that is fertilizing the soil. Ecology and concern for the environment came to me in practice. Of course, all of us cannot live on a farm; but surely, we don’t have to continue polluting the rivers and streams all the way to the Mississippi delta. Whew! Here I go again.
Thank you for being so prompt about the article on reparations. I really think Coates has given us a spiritual guide to bringing honor to the country for the ‘sins of our fathers’ as well as help for those who suffered some form of slavery or segregation that assured less opportunities for them than those of fairer skin.
Yes, I am hoping we can make progress in merging the two groups.
Doug
I certainly agree with you that human progress is not steady, it fluctuates up and down, but slowly rises overall. As the end result (so far) of evolutionary processes, I am mostly amazed that human civilization has a cultural and moral component beyond survival of the fittest. To me this is one sure sign of human progress. Of course, we have a long way to go but everything has to develop by trial and error and therefore takes a long time with many twists and turns along the way.
In short, I would say that I am taking an objective, impersonal, view of human cultural and moral development while you are taking a subjective and personal view.
Jack,
I wrote a comment but it may not have been sent. I’ll try to repeat it. Yes, I think you have made a good assessment of our points of view and that you view yours as objective and mine as subjective. I think you are kind of right. But I don’t think we can ignore the subjective. I understand your field of study is mathematics. I know very little in that area not much more than balancing my checkbook. My field of study is primarily the History of Ideas.I also understand that numbers are abstract that is they are adjectival nouns that refer to an object. Still, those abstract numbers require an individual to put on the drawing board. Now I will make a quick jump. I believe we use our senses to feed our intellect which is a concept not a fact. But I believe you use a theory also that is not a fact.
Here we get into a long philosophical struggle with such ideas as logical positivism, empiricism, rationalism, Darwinism, Evolutionary theory …etc.
Some of these concerns I will be addressing at the Tolerant Atheist Group on March 10. I hope you can attend. It might be fun.
Doug
I’ll be there, Doug, on March 10!
Jack,
.
The data regarding a person’s direct financial involvement in their own healthcare should also be assessed by its participation in the over-all change in the level of resources devoted by our nation’s economy to healthcare. I am aware that the cost of our nation’s healthcare was 6% of the GDP in 1960 and has been estimated to be 18% for 2015. For 2013, the other developed nations (a UN term) of the world spent less than 12% of their economy on healthcare, with generally accepted better levels of effectiveness. Its possible that our nation’s healthcare is inefficient to a level of 33%. Its also possible that obesity, lack of exercise, lack of jobs need remedies to bring the excess cost of healthcare to 25% of its current cost, estimated to be $3.3 Trillion in 2015. So, the excess cost of healthcare was $800 Billion of which the Federal government paid 40% for Medicaid and Medicare. I also understand that our nation’s government ran a deficit of $530 Billion in 2015. So, the excess cost of our nation’s healthcare amounted to 60% of that debt. I am not sure that any new concept for paying for the cost of our nation’s healthcare will substantially change this problem. Henry Aaron, an economist with the Brookings Institute, has estimated that by 2020 our nation’s debt per citizen will be the same as it is in Greece, now. Absolutely, “It doesn’t add up!”
.
Paul
This is a good analysis of how excessive costs of American healthcare, both public and private, relate to our out of control federal deficits. Sixty percent of the deficit can be attributed to just waste and inefficiency of Medicare and Medicaid alone!
The only way to achieve such big cost savings is to make fundamental changes in our overall healthcare system. This is what I’m trying to get at in my post above.
Lets assume that a Constitutional Convention was convened by the States, and it approves a Constitutional Amendment to require a “National Balanced Budget” annually. It should require accrual rather than cash accounting rules. I am aware that there is a national institution that defines these rules for our economy. But, its legitimacy might be problematic for the Federal government.
Of course, the issue for healthcare reform comes to this: how do we “rein in” 50 years of Parkinson’s Law as represented by Medicare and Medicaid? This law is defined as follows: In complex institutions “Work expands so as to fill the time (viz., resources) available for its completion.” Our nation’s future autonomy within the world-wide market-place arenas of resources, knowledge and human dignity is at stake based on improving the efficiency and effectiveness of our nation’s healthcare.
I think that you are raising reservations about a BBA. For sure it would be a huge shock to have to implement such an Amendment abruptly in the course of a single year. But there are ways to soften the blow, so to speak.
One way is for Congress to propose a BBA itself as we get closer to the 34 states required for a Constitutional Convention. I would actually expect Congress to do this. An amendment proposed by Congress would most likely be more flexible than one drawn up by a CC.
Another “softener” would be an emergency clause, sure to be included, that a 2/3 or perhaps 3/5 majority of Congress could override the strict balance requirement. Such an override provision would not be a problem, in my opinion, because the goal is not absolute balance, but approximate balance, which would still reduce the debt as a percentage of GDP over time.
You’re entirely correct though, that healthcare costs being the biggest driver of debt, then healthcare costs would become the biggest target for restraining costs under a BBA.