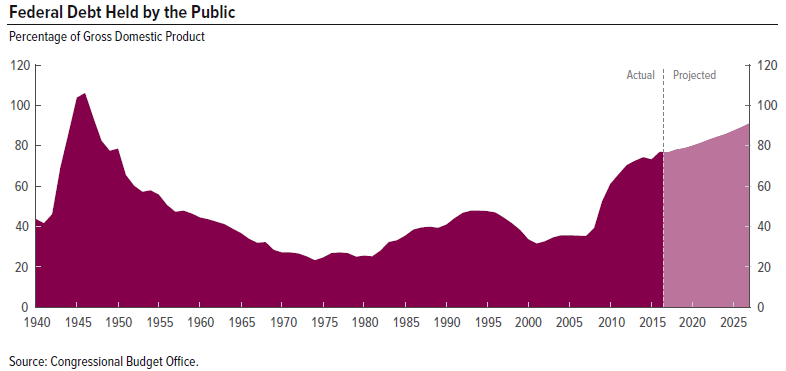
I am a candidate in the May 15 Nebraska Republican Primary for U.S. Senate, against the incumbent Deb Fischer because she is totally ignoring our enormous and out-of-control national debt. In fact she has just recently voted twice to make it worse than it already is.
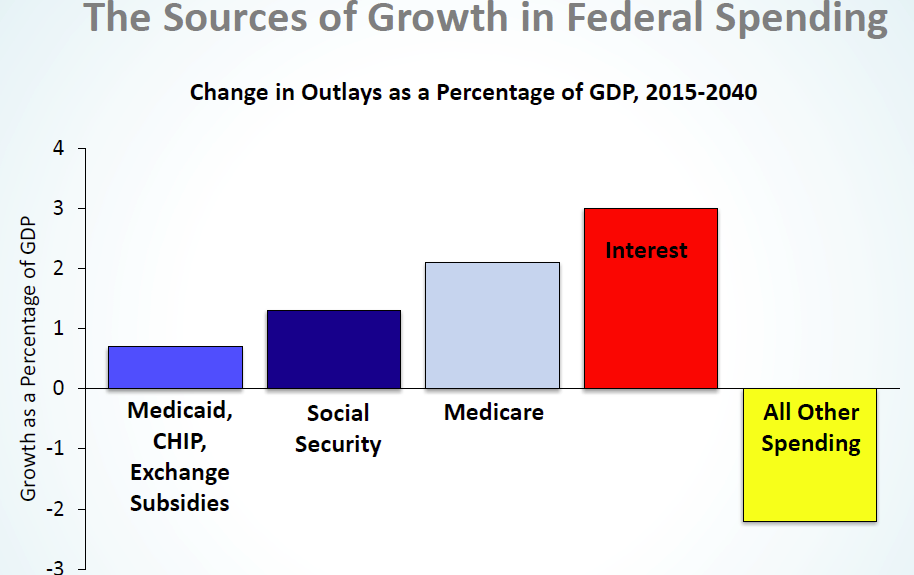
The major driver of our debt is the entitlement programs, Social Security, Medicare and Medicaid. Social Security is self-funded from the payroll tax and can be shored up long term with some relatively simple adjustments such as raising the income cap on which the payroll tax is levied and/or SLOWLY raising the eligibility age for full benefits. Medicaid costs can be controlled by block-granting it to the states with a fixed contribution from the federal government.
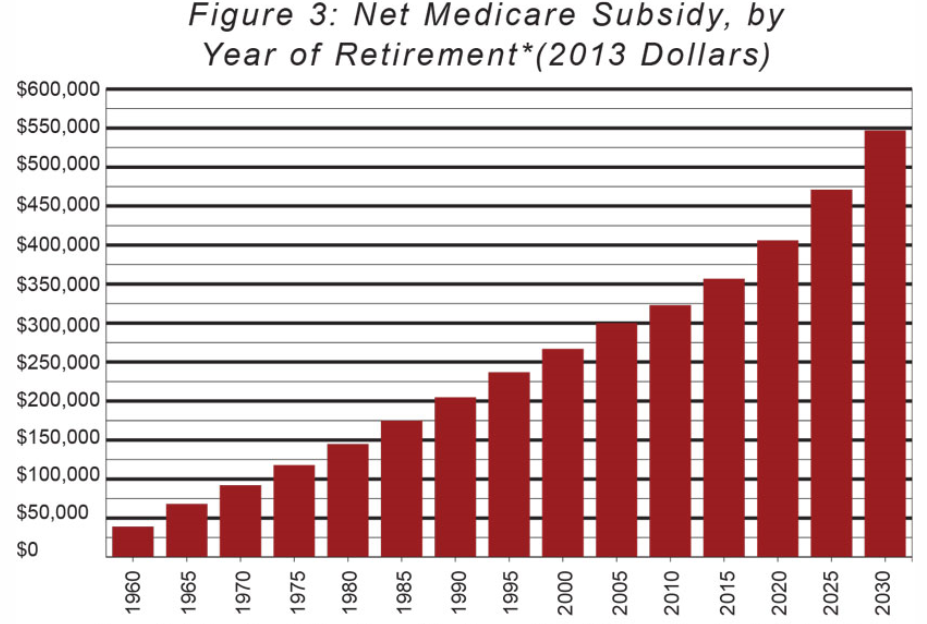
But Medicare will be much harder to reform because it is the most expensive entitlement program of all. The above chart shows that a couple with average wages reaching age 65 in 2015 can expect to receive Medicare benefits that exceed what they put in by $357,000. This subsidy will only increase in the years ahead.
The American Enterprise Institute’s James Capretta has recently described one possible way to get Medicare costs under control. In outline:
- Combine hospitalization (Part A), outpatient services (Part B) and drugs (Part D) into a single combined insurance product.
- Offer community-rated premiums for beneficiaries, meaning that premiums would not depend on age or health status.
- A small, universal entitlement benefit would be paid to all enrollees set to cover about 20% of today’s benefit and equal to about $2600. The Medicare payroll tax of 2.9% would pay for this universal benefit.
- Additional financial support would be based on lifetime earnings, with the lowest quartile receiving substantial additional support which would be phased out for middle- and upper-middle class retirees.
- Retirees would purchase private insurance plans which could be in the form of high-deductible catastrophic insurance combined with health savings accounts.
Conclusion. “The reform of Medicare outlined above is a plan to substitute higher premiums from the middle and upper classes for the large general-fund subsidies taxpayers now provide to Medicare to finance the majority of Part B and Part D costs. The end goal is a self-financing Medicare program.”