My last post, “Progress on Medicaid Reform,” discusses innovations that several states have adopted to improve the delivery of Medicaid and to make it more cost efficient. But what we really need is a complete overhaul of American healthcare, including the Affordable Care Act, as I have also recently discussed, in order to eliminate perverse marketplace incentives as well as to achieve real cost control.
 An excellent discussion of what real healthcare reform would look like is given by John Goodman in, “Healthcare Solutions for Post-Obamacare America.” Mr. Goodman gives six principles for commonsense reform:
An excellent discussion of what real healthcare reform would look like is given by John Goodman in, “Healthcare Solutions for Post-Obamacare America.” Mr. Goodman gives six principles for commonsense reform:
- Choice. People should be free to choose a health plan that fits individual and family needs, rather than one designed by bureaucrats in Washington. This means no mandates, either for individuals or employers.
- Fairness. Any subsidy should be in the form of a fixed sum tax deduction or credit and everyone should get it as long as they obtained credible private health insurance. The amount of the subsidy would be comparable to the cost of Medicaid enrollment.
- Universal Coverage. Since some people will turn down the offer of a tax credit, unclaimed credits can be used to reimburse safety net healthcare institutions.
- Portability. Portability insurance should be available to employees in case they change jobs or become self-employed.
- Patient Power. Health Savings Accounts need to be made more available and also more flexible so that they can wrap around any third-party insurance plan, as indicated in the above chart.
- Real Insurance. Under ACA millions of people are losing access to out-of-network providers. People should be allowed to purchase “change-of-health-status insurance” in case they develop expensive-to-treat conditions.
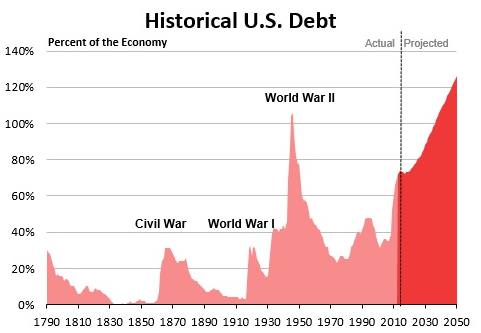
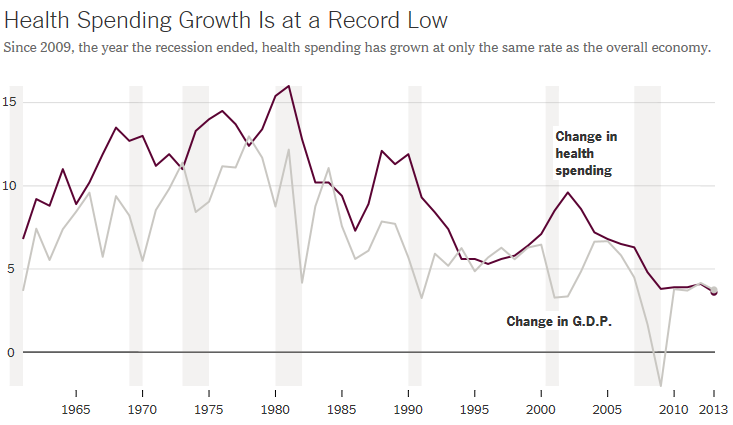
The ACA addresses the access problem for healthcare but has little effect on the cost problem. American healthcare, both public and private, is way too expensive. This is why fundamental change is still needed.