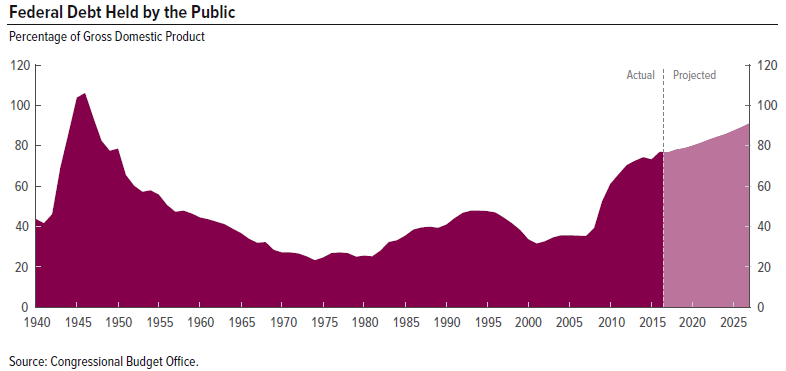
The Affordable Care Act, established in 2010, greatly expanded access to healthcare in the U.S. However, in spite of its name, it has done nothing to control the rapidly increasing cost of healthcare which is the core of our debt problem.

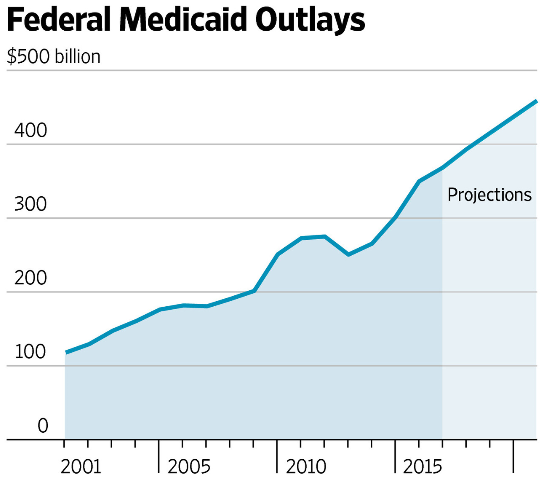
The new Senate plan, struggling to gain enough support to pass, puts Medicaid on a budget but doesn’t even attempt to address wider aspects of the healthcare cost problem.
A wider approach is the best way to proceed and perhaps now it is the only way to succeed in getting something done. Mr. Peter Suderman, who writes for Reason magazine, proposes several principles for a new approach:
- Work for broader coverage but not necessarily universal coverage. This allows focusing on other important features such as:
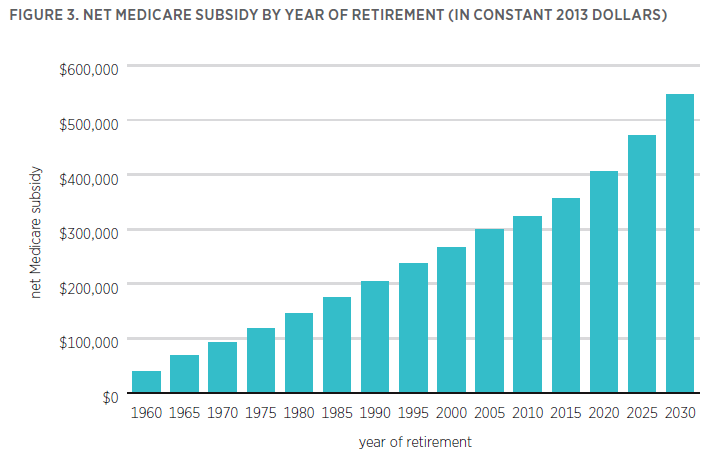
- Unification, not fragmentation, is what should be emphasized. Medicare and Medicaid are paid for directly by the government. Employer provided coverage, subsidized through the tax code and costing $250 billion per year, is the biggest problem in the U.S. healthcare system. It incentivizes employers to provide ever more generous insurance while insulating individuals from the true cost of care. It discourages job switching and entrepreneurship. Medicare ends up paying out far more than individuals have paid in.
- Health insurance coverage is not the same as healthcare. For non-catastrophic, non-emergency expenses, affordability should be emphasized, rather than subsidies. Health savings accounts are a good way to accomplish this.
- Focus on government assistance for the poorest and sickest. This means upgrading Medicaid, and coverage for pre-existing conditions, at the same time as putting Medicaid, Medicare and employer provided care all on a fixed, but reasonable, budget.
Conclusion. The cost of American healthcare is a huge problem. Hopefully the Senate will begin to address this fundamental problem as it struggles to pass a healthcare reform bill.
Follow me on Twitter
Follow me on Facebook