Recently I have been discussing the high cost of American healthcare and the urgent need to lower this cost. The current GOP plan, the American Health Care Act, partially addresses this problem by reforming the funding mechanism for Medicaid.
But much more needs to be done. All Americans will have to be involved in the solution and not just the poor. There are two main facets to the problem, neither of which is addressed by the AHCA:
- The tax exemption for employer provided health insurance should be replaced by a universal (and refundable) tax credit limited to the cost of catastrophic health insurance (with a high deductible).
- Medicare needs to be redesigned so that well-off retirees pay for more of their health care. Details to follow soon.
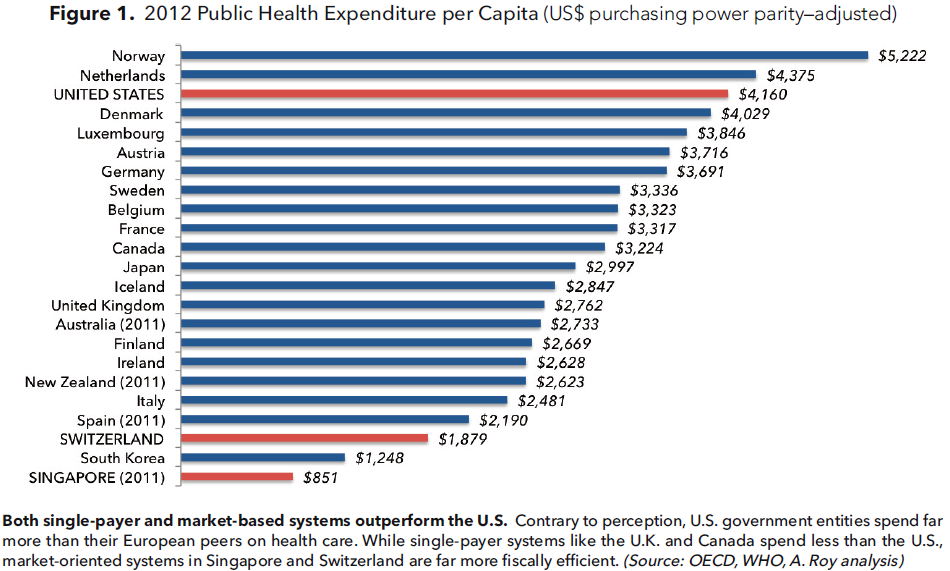
The U.S. spends 18% of GDP on healthcare, public and private, about $3 trillion per year, and almost twice as much per capita as any other developed country. Furthermore this already enormous relative cost will continue to get worse without major changes in policy.
The main reason for the huge cost is that free market forces are not operating properly. More specifically, it is because most of us, as individual healthcare consumers, do not have enough “skin in the game.”
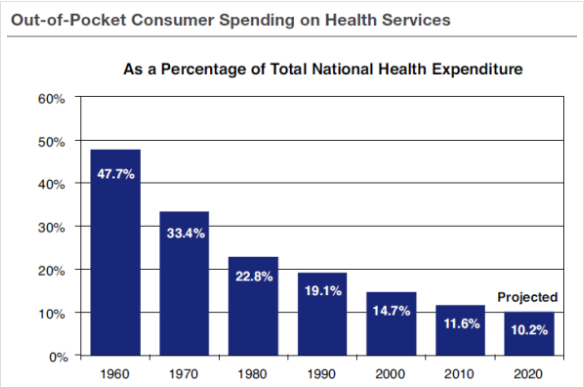
This conundrum is caused by our third party health insurance system whereby most of us receive health insurance through our employers. This gives us as individuals little incentive to pay attention to the cost of our own care and to try to keep these costs as low as possible.
A good way to fix this problem is to limit the exemption for employer provided insurance to the cost of catastrophic care with a high deductible. Routine medical expenses would be handled through individual (tax preferred) health savings accounts. The self-employed can be included by granting them a (refundable) tax credit also equivalent to the cost of catastrophic care.
Conclusion. Americans are fortunate to have access to high quality health care. But we are paying unsustainably high prices for it. If we cannot figure out a rational and sensible solution to this problem, our healthcare system will soon collapse from its own deadweight and we will end up with a tightly controlled, government run, single payer system.