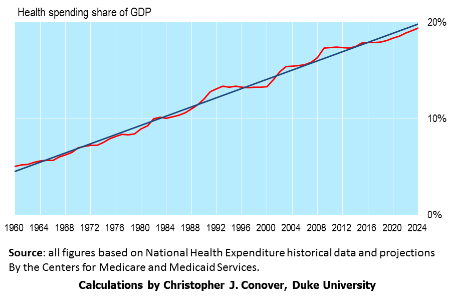
U.S. healthcare policy is now in limbo. The Affordable Care Act has withstood Congressional attempts to repeal it, but it has many flaws which need to be repaired. Primarily, the ACA expands access to healthcare in the U.S. (good) but does nothing to control burgeoning costs for both individuals and the federal budget (bad).

One option for both further expansion of access as well as cost control is Bernie Sanders’ single-payer “Medicare for All” plan. A different option is universal catastrophic care for all Americans not already covered by Medicare or Medicaid (including those receiving employer provided health insurance).

A different perspective is provided by an editorial in the New England Journal of Medicine. According to the authors, Eric Schneider and David Squires, the U.S. also faces (in addition to the challenge of much better cost control) several performance challenges such as:
- Lack of access to affordable and comprehensive insurance coverage for too many people.
- Relative underinvestment in primary care. Other developed countries have a higher percentage of their professional workforces dedicated to primary rather than specialty care and deliver a wider range of services at first contact.
- Administrative inefficiency of the U.S. healthcare system. The solution here is to change our reimbursement systems to use global payments, fee schedules, formularies and defined benefits.
- Disparities in the delivery of care. People with low incomes, low educational attainment, and other social and economic challenges face greater health risks and thus need even greater access to primary healthcare.
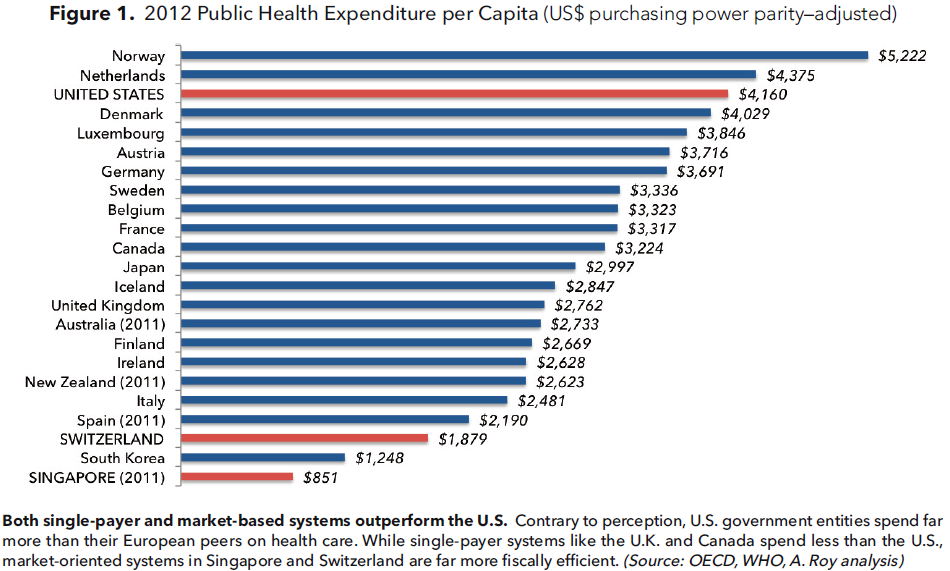
Conclusion. The U.S. compares poorly with other advanced countries in both the quality and cost efficiency of its healthcare system. Healthcare costs in the U.S, are a huge drain on the economy and will ultimately cause huge fiscal problems if not brought under much greater control.