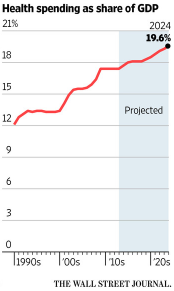
My last two posts, here and here, argue that the high costs of American healthcare, almost double what other developed countries pay per-capita, has two fundamental causes which must be addressed:
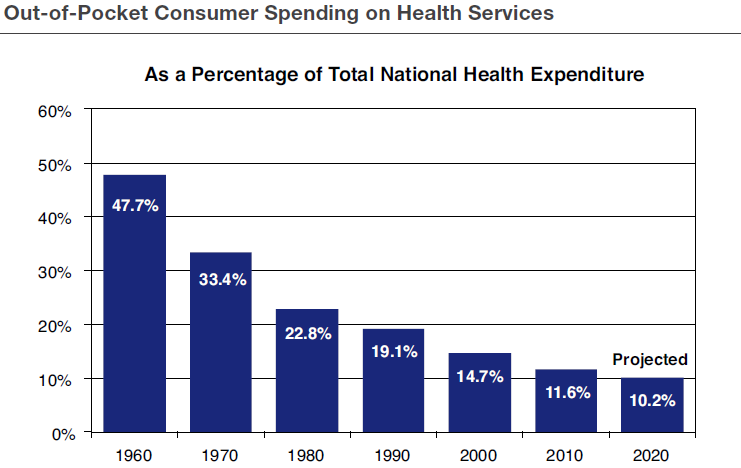
- Very low out-of-pocket costs as a result of the tax exclusion for employer provided care.
- The very expensive, and rapidly growing, government entitlement programs of Medicare and Medicaid.

It is often suggested that the best way to get these high costs under control is for the U.S. to adopt a single-payer, government run, healthcare system, like many other developed nations have done. Writing in yesterday’s Wall Street Journal, the policy analyst, Nathan Nascimento, makes a persuasive, and well referenced, counter argument to this suggestion:
- The State of Vermont recently backed away from implementing a single payer system because of the very high tax increase which would have been required, more than doubling Vermont’s annual budget.
- The State of Colorado will vote a year from now on a petition-supported single payer proposal, ColoradoCare, which would be paid for by a $26 billion annual state tax increase and is therefore unlikely to pass.
- In Canada, which has a single payer system, the average wait between a general practitioner’s referral and delivery of treatment was more than four months in 2013.
- Our own Veterans Affairs hospital system, a single payer system on an annual budget, is failing thousands of veterans who often die while waiting for treatment.
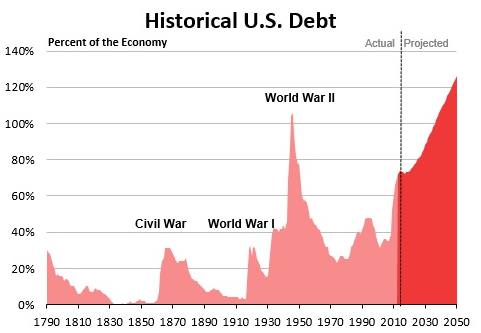
- Medicare, an open ended single payer entitlement system, now costing almost $600 billion per year, is one of the main causes of our burgeoning, out of control, national debt.
Conclusion: For the U.S. to move to a national single payer system would be very risky and very costly. It is far better to wait and see if Colorado or some other state is willing to take such a leap of faith and then see how it works out in that context.
Follow me on Twitter: https://twitter.com/jack_heidel
Follow me on Facebook: https://www.facebook.com/jack.heidel.3