My last two posts, here and here, have made the case that:
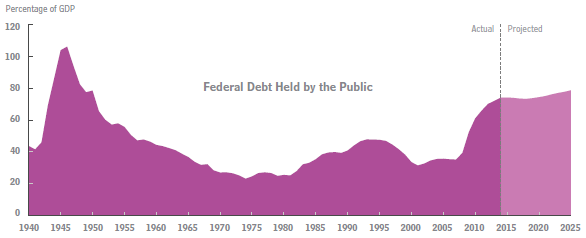
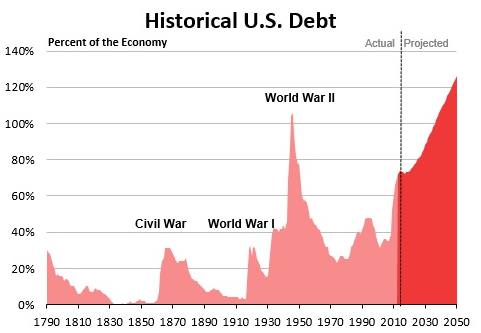
- Our national debt is now 74% of GDP (for the public part on which we pay interest), the highest since WWII, and steadily getting worse. This will create a huge problem in the not so distant future, as soon as interest rates return to normal (higher) levels.
- Entitlement spending is the main driver of our increasing debt. The best way to control Medicare and Medicaid spending is to control the cost of health care spending in general.
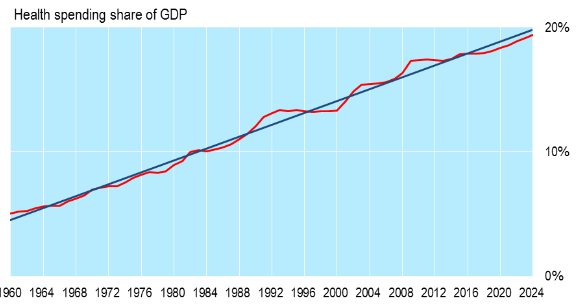
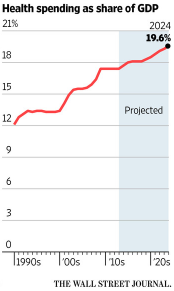
- The overall cost of health care, public and private, in the U.S. is now 17.4% of GDP, much higher than for any other developed country, and is steadily increasing.
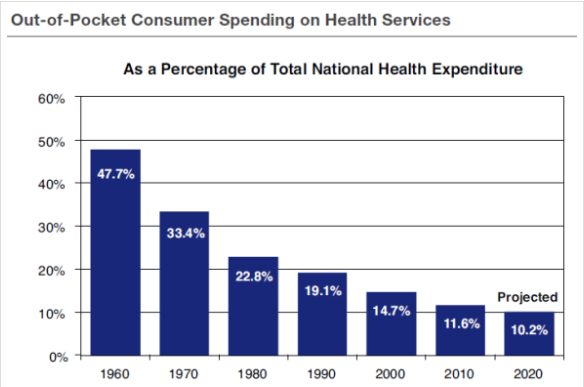
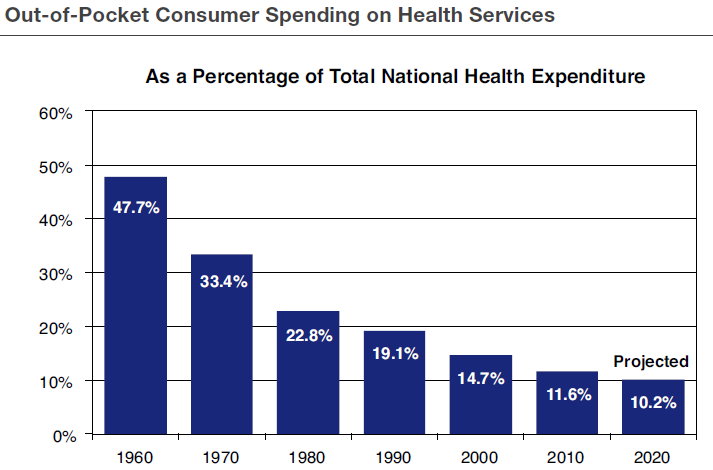
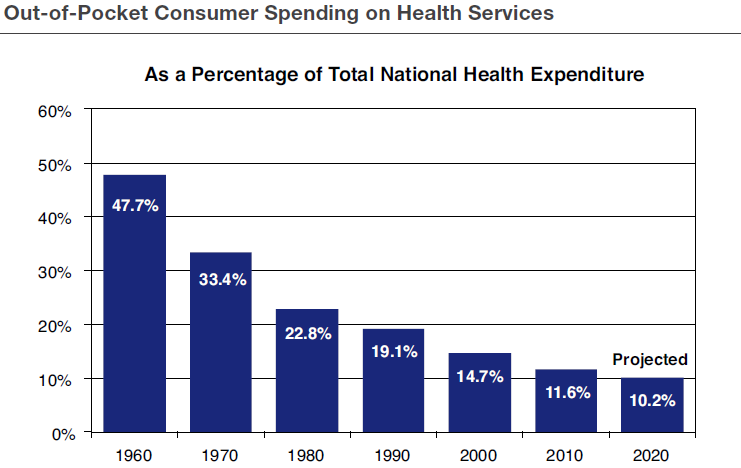
- The main reason our health care costs are rising so rapidly is that Americans do not have enough “skin in the game.” Health insurance pays for close to 90% of our health care costs so that we pay for very little directly out of our own pockets. This means we have little incentive to pay close attention to these costs.
Christus Health in Dallas and Privia Medical Group in Washington, DC are causing disruption by shifting health care delivery from hospitals to outpatient settings. They are putting in place a number of lower-cost and more consumer friendly options which reward collaboration, performance and a focus on cost and quality on the part of both management and front-line providers.
 As I have pointed out in previous posts, here and here, several policy changes would help speed up this process of needed change:
As I have pointed out in previous posts, here and here, several policy changes would help speed up this process of needed change:
- The tax exemption for employer provided health insurance should be limited to the cost of high deductible catastrophic insurance with an equal (refundable) tax credit for those without employer coverage. Health Savings Accounts would be encouraged for routine health care expenses.
- Affordable Care Act exchanges would continue to operate as at present but without any mandates.
- Medicare would provide a fixed level of assistance with which seniors would purchase a private health plan of their own choosing, rather than being open ended as at present.
Medicaid. The federal government would give states fixed, per-person payments. Low-income individuals could combine Medicaid and the (refundable) tax credit to enroll in private insurance.
Conclusion. The whole idea is to make everyone, rich and poor, young and old alike, responsible for their own health care expenses. Only with such a consumer-oriented, free-market system will we be able to preserve the high quality of American health care and rein in excessive costs at the same time.