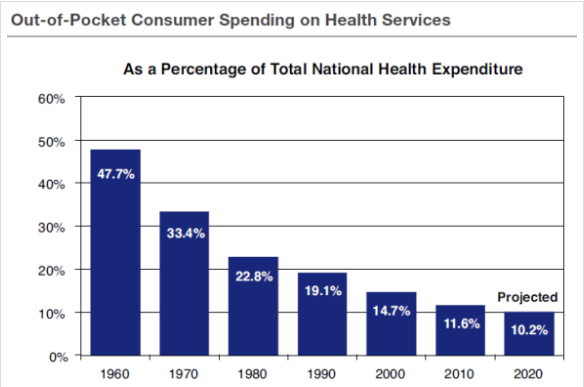
One of the major problems facing the United States today is the high cost of healthcare. We spend almost 18% of GDP on healthcare, both public and private, almost twice as much as any other developed country. A big reason for the high cost is the low out-of-pocket consumer spending on health services in the U.S.
My last post discusses a general plan, involving catastrophic health insurance and health savings accounts, for getting the overall cost of healthcare under control.
 Once we have a handle on the overall problem, we then need to focus on the cost of the Medicare entitlement program for retirees. The problem here is easy to understand. In just 15 years enrollment in Medicare will increase to over 80 million beneficiaries from 57 million today. Likewise there are 3.1 workers per beneficiary today and there will be only 2.4 in 2030 (see above chart).
Once we have a handle on the overall problem, we then need to focus on the cost of the Medicare entitlement program for retirees. The problem here is easy to understand. In just 15 years enrollment in Medicare will increase to over 80 million beneficiaries from 57 million today. Likewise there are 3.1 workers per beneficiary today and there will be only 2.4 in 2030 (see above chart).
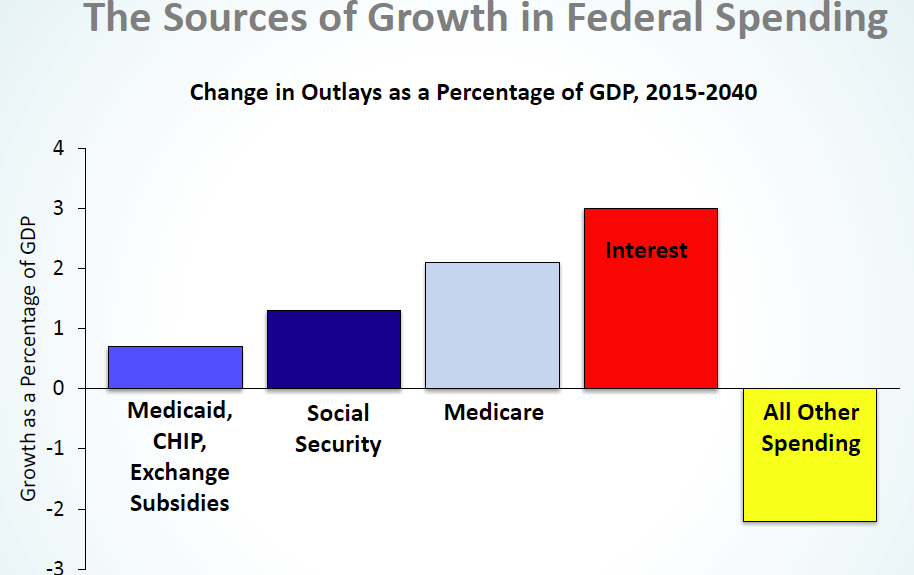
The second chart demonstrates that Medicare will be the major component of increases in federal spending in the coming years (with the other entitlements of Social Security and Medicaid following right behind).
So the question is: how do we control Medicare spending within the context of overall health-care reform? Here is a proposal from James Capretta of the American Enterprise Institute:
- Medicare recipients would receive fixed payments toward the coverage option of their choice, based on their age, income and health status. The traditional Medicare program would be one of the choices. Enrollees choosing less costly coverage options would see a reduction in their premiums.
- Premium payments would be comparable to subsidies and tax credits received from the reformed Affordable Care Act.
- Privately run managed care plans provide benefits at far less cost than traditional Medicare. Beneficiaries would share in the savings.
Conclusion. It needs to be emphasized as strongly as possible that the point of Medicare reform is to lower costs to both individuals and the government, sa that Medicare can be preserved indefinitely into the future.