
As I discussed in my last post, it is critical and urgent for the U.S. to sharply reduce the cost of healthcare, both public and private. There are basically two different ways to do this: with either a “single payer” system like most of the rest of the developed world has, or with a more nearly free market system than we have at the present time.
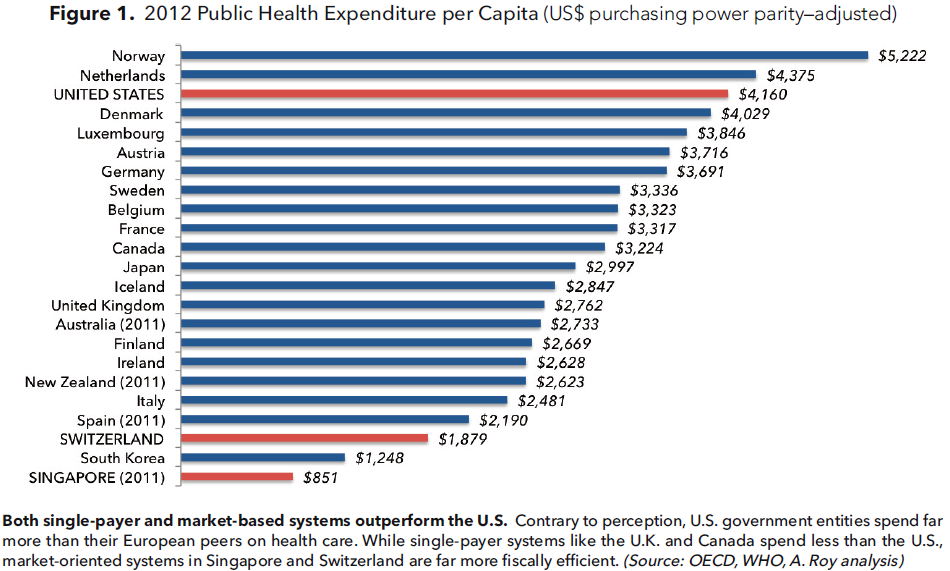 Both Switzerland and Singapore have largely free market systems with universal coverage and they operate at far less public cost, as shown above, than for other developed countries including the U.S. The Singapore model features Catastrophic Care insurance, coupled with Health Savings Accounts, for all citizens, with subsidies for those with low-income. The Swiss model employs exchanges, similar to our own Affordable Care Act, to subsidize, on a sliding scale, health insurance for the low income. In Switzerland only 20% of the people receive an insurance subsidy compared to 85% in the U.S.
Both Switzerland and Singapore have largely free market systems with universal coverage and they operate at far less public cost, as shown above, than for other developed countries including the U.S. The Singapore model features Catastrophic Care insurance, coupled with Health Savings Accounts, for all citizens, with subsidies for those with low-income. The Swiss model employs exchanges, similar to our own Affordable Care Act, to subsidize, on a sliding scale, health insurance for the low income. In Switzerland only 20% of the people receive an insurance subsidy compared to 85% in the U.S.
The Manhattan Institute’s Avik Roy has proposed a true free market system for the U.S., “Transcending Obamacare: a patient-centered plan for near-universal coverage and permanent fiscal solvency,” which is modeled on the Swiss system. Mr. Roy’s plan sets up universal exchanges to offer insurance, subsidized if necessary, to everyone who does not receive it from their employer.
He proposes that over time Medicare and Medicaid recipients as well as Veterans would migrate into the exchange system. This means that eventually the 30% of Americans (elderly, poor and veterans) who now receive direct government (single payer) support would become part of the exchange system. Mr. Roy’s Universal Exchange Plan is projected to reduce deficit spending by $8 trillion over the 30 year period which it will take to fully phase in the exchanges. This will go a long way towards solving our serious fiscal problems.
Conclusion: both Singapore and Switzerland have high quality, cost efficient free market health care systems which proves that a free market approach is possible. Mr. Roy adapts and expands the Swiss model for the much larger and more complex American market. It isn’t necessarily the last word in healthcare reform but it takes a big step in the right direction.






